


Might a community approach be one of the solutions for social distancing, the scope of which has been revealed by the current pandemic? This is the argument put forward by the three authors, members of Médecins du Monde Canada.
The lack of preparation in Western countries, which has been universally acknowledged, has been even more strongly felt in the impact of the Covid-19 pandemic on the poorest, most marginalised people in our societies. These include migrants, economically precarious populations, homeless people, drug users, and sex workers. The measures and practices adopted in response to the disease have exacerbated financial insecurity, domestic violence, stigmatisation, and pre-existing psychological problems amongst these groups. Moreover, in this context of mandatory “distancing”, they have become even more inaccessible.
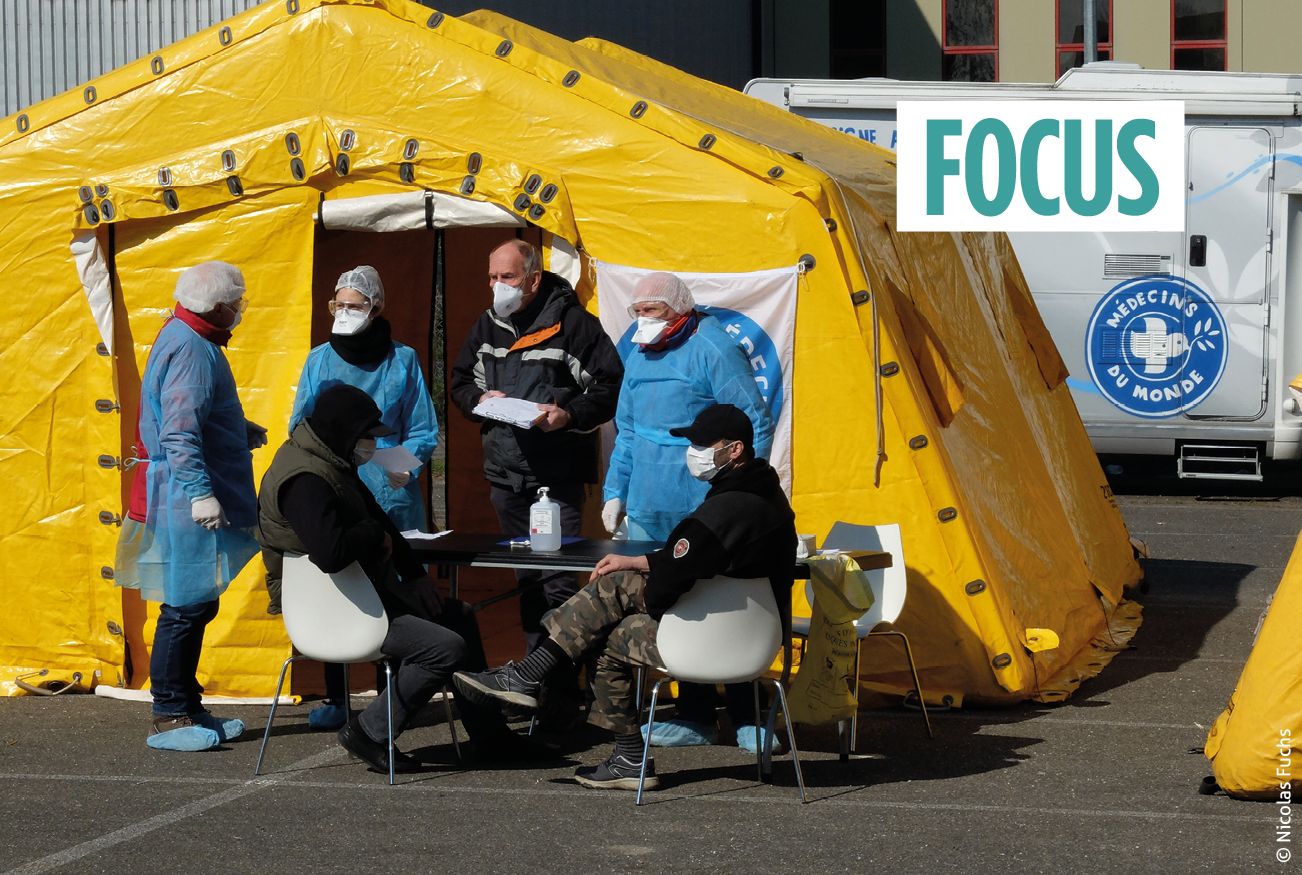
The health and safety measures adopted to fight against Covid-19 also exacerbate exclusion and instability.
These factors of insecurity are clearly significant in a situation where it is imperative to appeal to international aid, especially since there has been a general trend of community suspicion and lack of confidence towards foreign NGOs and their international staff. Projects face obstacles in the countries of intervention relating to reduced access and changing realities, as much from a social point of view as from a political and economic one.
Médecins du Monde therefore found itself compelled to adapt its programmes, not only in international contexts but also in local ones. The common point between these different situations is the community health approach, so dear to Médecins du Monde, which is proving to be absolutely essential at this time, both in preventing and fighting against the disease itself as in enabling communities and health systems to overcome this crisis. Beyond humanitarian organisations, these lessons could undoubtedly also be applied to the orientation of multilateral health development programmes, and to health systems here and abroad.
Covid-19 as revelatory of inequalities, and as an aggravating factor
The people most at risk of contracting Covid-19 have been identified as the elderly, those suffering from chronic illnesses, the immunocompromised, and poor or marginalised people[1]Public Health Agency of Canada, “Vulnerable populations and COVID-19”, 25 May 2020, available online: … Continue reading. Our health systems, and especially in Canada, have focused on actions in favour of the first three groups, leaving those from the last category behind. And yet we can see the extent to which the current pandemic has exacerbated their situation and the inequalities with which they are faced.
Indeed, across high-, middle- and low-income countries, this virus particularly affects people living in poverty and whose state of health is compromised due to their lack of resources and access to health services. Hence, homeless people, those living in overcrowded accommodation or working in conditions where physical distancing is impossible (because they do not have access to protective equipment) are more likely to contract Covid-19[2]P. Tircher and N. Zorn, « Inégaux face au coronavirus. Constats et recommandations », Observatoire québécois des inégalités, Montréal, 2020, p. 8, available online: … Continue reading. Moreover, their state of health is often initially worse than the general population, and the presence of comorbidities represents an added risk, making them more vulnerable to the disease.
The health and safety measures adopted to fight against Covid-19 also exacerbate exclusion and instability. In many situations, the public health requirements have actually led to a reduction or cessation of the activities and services of community and humanitarian organisations that ordinarily meet these populations’ essential basic needs. Moreover, beyond losses of jobs and income, tightened security at the borders and in the public sphere, as well as repressive regulations on social conduct, represent a double penalty for people in marginalised situations. The pandemic has exposed a society with different “lanes”, where some people have the means to protect themselves and to comply with regulations, whilst others are penalised for their inability to do so.
Covid-19 as revelatory of the weaknesses of our health systems
The pandemic does not only affect individuals’ health. It has also destabilised institutional frameworks, revealing the gaps created by policies which have ultimately weakened health systems and communities, making them more vulnerable to Covid-19 and its consequences. We could take the example of user fees in healthcare, which have long been a mainstay of the World Bank and the International Monetary Fund’s development policies for health systems, but which, without strong community management, have proven to be extremely damaging in crisis contexts[3]Robert Yates, “In the Covid-19 Era, Healthcare Should be Universal and Free”, Chatham House, 11 May 2020, … Continue reading. In the same way, interventions leading to the increased institutionalisation of services create numerous obstacles between the population and the health system.
Policies aiming to centralise and homogenise health systems have also turned out to be highly detrimental in this pandemic context. The example of Quebec is very revealing on this point. Years of reforms to centralise the system, streamline the administration and encourage mobility amongst personnel in order to reduce associated costs[4]Institut national de santé publique du Québec, « Évaluation de la mise en œuvre du Programme national de santé publique 2015-2025 – Analyse de l’impact des nouveaux mécanismes de … Continue reading have placed its metropolis, Montreal, at the top of the list of global mortality rates associated with Covid-19[5]Comparaisons santé : Québec/Canada/OCDE, « Mortalité par Covid-19 au Québec : comparaisons nord-américaines et internationales. Mise à jour du 15 juin », … Continue reading. Caught in a “streamlined” system structured around mega-organisations, health and care institutions found it difficult to react promptly and adequately in the face of the pandemic. The Ministry of Health and Social Services in Quebec was eventually forced to hire a significant number of volunteers, who were untrained and sometimes under-supervised, in order to make up for the lack of personnel in old people’s homes, and then to ask for the help of the Canadian Army and the Red Cross to fight on this same front. Likewise, more than two months after the declaration of a health emergency, health personnel were continuing to move between non-Covid-19 and Covid-19 areas, even though this mobility was acknowledged to be extremely conducive to the spread of the virus.
Community health as one of the possible solutions
Faced with this pandemic, what it reveals about our societies and its impact on the most vulnerable populations, a community approach to healthcare seems to us to be more relevant than ever, here in Canada and elsewhere. Indeed, this approach provides a corrective to an important shortcoming in the actions undertaken in the fight against the epidemic: the social and anthropological dimension is too often ignored, whereas it requires a comprehensive approach, in accordance with the cultural context[6]Jean-François Delfraissy, Benoît Miribel, “Lessons from Ebola”, Humanitarian Alternatives, inaugural issue, p.22-27, http://alternatives-humanitaires.org/en/2016/01/17/lessons-from-ebola.
Whilst it is not possible to draw a complete parallel between the two health crises, the measures which enabled us to check the spread of the Ebola epidemic, which ravaged West Africa from 2013 to 2016, can guide how we respond in the face of the crisis that we are currently experiencing[7]For more detail on the lessons drawn from the management of the Ebola virus, see also the article in this issue by Stéphanie Maltais, “Learning the hard way: how the Ebola virus experience can … Continue reading. Secure and accessible treatment centres, monitoring and contact tracing, the safe and dignified management of deaths, as well as awareness-raising amongst and involvement of the populations, which were put in place at the time, all proved to be determining factors in bringing the then-raging epidemic to an end.
In Liberia, it was shown that the setting-up of decentralised community healthcare centres was a key factor in limiting community transmission of the virus. In the same way, the rapid deployment of a response to the Ebola virus at the community level was shown to be both possible and effective[8]Paul Pronyk et al., “The Effect of Community-Based Prevention and Care on Ebola Transmission in Sierra Leone”, American Journal of Public Health, 106(4), April 2016, p.727-732, … Continue reading. Also in Liberia, it turned out that the formal and informal strategies of local communities in certain urban areas succeeded in bringing the epidemic under control, in spite of systemic failures on the part of States and the international community. In the absence of health support, infrastructures and equipment, communities therefore became self-sufficient in order to contain the epidemic at a local level[9]Sharon Alane Abramowitz et al., “Community-Centered Responses to Ebola in Urban Liberia: The View from Below”, PLoS Neglected Tropical Diseases, 9(4), 9 April 2015, … Continue reading.
These lessons confirm the relevance of a community approach in the health sector, which has long been promoted by Médecins du Monde. The organisation notably favours awareness-raising and the involvement of the community, investment in community health agents and primary care providers, empowerment and the fight against stigmatisation, and finally, a refusal of the hierarchisation of knowledge. This approach is at the heart of our mission, especially when we are working alongside marginalised populations. Linking individuals and communities where they are and when they need it remains a central aspect of these programmes. Mobile clinics, community rounds, general support: it is the service that travels and adapts itself to the person and their environment, and not the other way around. Although we are aware that it is sometimes difficult to transpose these models, tailored to the scale of a Canadian province, it is our belief that the confidence and deep ties to the communities which they create should guide us with regard to which dispositions to adopt in our health services and in our interventions on an international scale.
Resistance in the face of long-term, paradigmatic change
A true community health approach requires the involvement of ordinary citizens for the development of the intervention, decision-making at all stages of the process (especially to adjust interventions throughout the implementation) and the evaluation of said process. Encouraging this involvement necessarily requires proximity to the people concerned. Yet international NGOs, which are responsible for significant financial resources, indebted to their sponsors and invested in the promotion of knowledge and best practices implemented in other contexts, often find themselves caught between their own bureaucratic rigidity and the need to operate with a certain flexibility.
The debate on the localisation of humanitarian action took off during the World Humanitarian Summit in 2016. This acknowledgement of local actors’ skills is not only morally and ethically sound, but it is also the right direction to take because localisation increases the impact of interventions and improves their efficacy. Nevertheless, it is estimated that less than 2% of humanitarian aid is allocated to local NGOs, and a paradigm shift must involve a better power balance and better distribution of resources[10]For more detail on localisation and the potential impacts of Covid-19 on its effective implementation, see the article in this issue by Martin Viélajus and Jean-Martial Bonis-Charancle, “Aid … Continue reading.
The full acceptance of a participative approach to community health gives rise to another form of resistance: the hierarchisation of knowledge. By way of example, with regard to interventions for basic health needs, this is especially noticeable in programmes for maternal and infant health. In Haiti, where MdM Canada is present, the institutional health system tends to adopt a utilitarian view of traditional midwives. They are considered as mere go-betweens for institutions, and their knowledge and input are not valued. This attitude betrays an ignorance of their role for women and the esteem in which they are held. Sidelining them from actions aiming to reduce the mortality rate amounts to being unable to understand barriers to access and resistance to giving birth in hospital environments.
To give another example of the importance of taking field experience into account, we might mention the issue of peer integration in the development of care pathways. This approach is part of an intervention dynamic based on the proximity between the individual leading the intervention and the person benefiting from it. This has proven to be particularly relevant in “harm reduction”[11]Harm (risk) reduction stems from efforts in the 1980s to try to limit HIV transmission amongst users of psychoactive substances. It involves the implementation of measures such as programmes for … Continue reading projects aimed at users of injectable or inhalable drugs – the aim being to create conducive conditions to anchor frontline services in the needs and realities of the people they are treating. Indeed, a lack of understanding on the part of health professionals can lead certain people to refuse to use the services available, and ultimately, to the deterioration of these people’s state of health.
Inclusive and participative approaches therefore often struggle with problems of representativeness in the target communities. It turns out that participants do not always represent the entire community in terms of social position and access to resources (certain groups have a stronger influence). Moreover, we can see that there are differing points of view between health professionals, and a perception that non-medical participants have neither the ability nor the required knowledge to discuss or opine on certain subjects. Finally, a participative approach to community health destabilises existing power and decision-making relationships.
Towards social change
In the international humanitarian ecosystem, Médecins du Monde Canada is undoubtedly a modest actor, given its budgets, and the scale of the projects that it runs. This is far from being a disadvantage since this agility within our organisation and the proximity of our actions enable us to be present where no one else is. This way of doing things has proven fruitful, not only at the international level, but also at the level of our local actions. Committed to defending the rights of vulnerable people in our own societies, we draw our legitimacy from our primary health and mental health programmes and advocate in favour of changes to our health systems, which are often fossilised and technocratic.
The Covid-19 pandemic has reminded us that community acceptance and grassroots principles should be the fundamental basis of all our operations.
In these different contexts, the Covid-19 pandemic has reminded us that community acceptance and grassroots principles should be the fundamental basis of all our operations. As a humanitarian organisation working in the sector of health, we rely on people from “target communities”, who hold influence and legitimacy in the eyes of their communities and who have the necessary experience to adapt our interventions according to the realities on the ground. This proximity, which also requires an openness to the participation of the people involved, has seemed self-evident to us now for a number of years. The current global pandemic shows the extent to which a community approach to health must be at the centre of national and international responses.
Translated from the French by Juliet Powys
ISBN of the article (HTML) : 978-2-37704-678-2 |



